

Mass Timber in Healthcare Facilities
- Oct 16, 2020
- 6 min read
Updated: Nov 21, 2024

There is increasing emphasis across Canada and the world for the incorporation of mass timber as a primary structural material in building design. While North America has been slow in adopting this material, which has been in widespread use in Europe for decades, there has been a dramatic increase in its use in the US and Canada over the last few years. Canadian codes are now allowing up to 12 stories of mass timber construction.
New projects are being developed in mid-rise and multi-storey residential, student housing, post-secondary academic buildings, office, and commercial construction. These are in addition to the ongoing use of timber in schools, cultural facilities, and other areas. However, despite this swift rise, and its positive impact on sustainability, the use of mass timber in healthcare facilities has been slower to develop. Mass timber has been typically relegated to non-clinical areas, such as exterior canopies, lobbies, atria, and other public areas.
There, timber’s known biophilic properties, which we as humans are drawn to because they reflect nature and environments that have supported human life in the past, are used in creating healing or reassuring spaces. But its use in clinical areas has not been accepted.

The exterior canopy at Sechelt Hospital in British Columbia is an example of timber use in a non-acute area of a healthcare facility. Image found here.
Infection control requirements, especially now in the COVID-19 era, and moving into post-pandemic life, are becoming more important. The impact on long-term care facilities and related facilities, such as acute care facilities and seniors’ housing, will impact the functional design of these facilities.
This article seeks to explore how we might overcome the roadblocks to adopting the use of mass timber in the clinical areas of our healthcare facilities. These include structural systems, infection control, fire safety, and the use of combustible materials. As we reexamine the issues, with consideration of the additional concerns brought into the open by the pandemic, we will also address the positive case for timber, such as sustainability and carbon sequestration.
ROADBLOCK 1: STRUCTURAL SYSTEMS
Entuitive has completed a research project with Forestry Innovation Investment (FII) to study the structural systems that would meet the requirements to allow for timber as a building material in healthcare facilities. In this study, several flat ceiling hybrid floor systems were reviewed and analyzed to determine prototype structural systems that could meet performance requirements, including infection control.
Office buildings are typically built with large spans, often on a 9-metre grid. A number of mass timber systems and innovations have been developed to span these grids and deal with the structural challenges of strength and also of vibration and acoustics. Hybrid systems, including the use of steel or concrete elements, are key to the increased reach of the mass timber market into the healthcare realm. These systems have been developed to produce flat ceilings without dropped beams to help with the distribution of M&E services. These other elements are built in the same “layer” as the mass timber elements.

77 Wade Avenue in Toronto is an example of timber as a building material in a future commercial development.
These systems typically use mass timber panels acting compositely with concrete topping as the floor deck. In our study, various mass panel products were analyzed, including CLT, GLT, and DLT. These, and other panel products, are typically premanufactured in controlled environments using lumber laminations that have been kiln dried. This is critical for hybrid systems. Differential shrinkage between these organic elements and the flush elements, whether concrete or steel, must be minimized.
These floor panels are supported by flush beam systems and our study investigated both steel and concrete beam systems. With either, the column and beam elements are erected first. The floor panels are then placed on this support system. Finally, the concrete topping is placed to connect these elements together to create a monolithic system.
Specialized steel beam systems have been specifically developed to provide flush soffits. Similar concrete beam systems can be cast-in-place or precast. The study evaluates the advantages and disadvantages of each system and finds that viable structural solutions for mass timber systems that are currently available in the market can compete with traditional concrete construction.

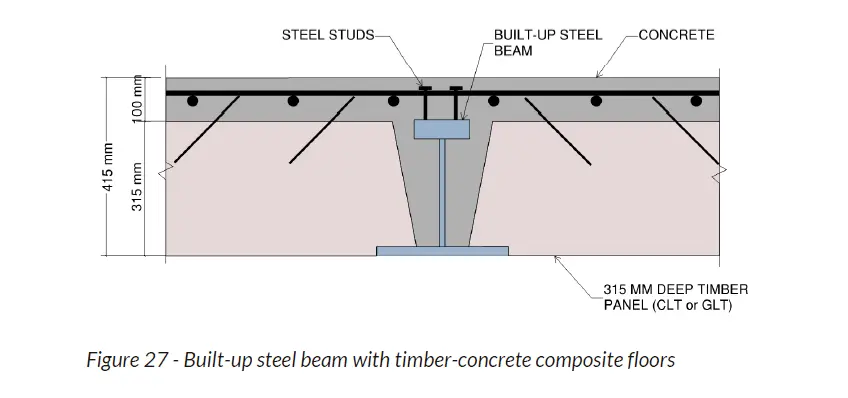
These figures, taken from a report produced by Entuitive for FII show the feasibility of timber from a structural point of view.
ROADBLOCK 2: FIRE PROTECTION
Fire protection for structures is obtained by protecting critical elements from damage to high temperatures. In concrete construction, minimum cover requirements over reinforcing steel serve to prevent excessive heat from reaching the reinforcing and causing it to lose strength. The same is achieved with steel structures using fireproofing spray, intumescent paint, or encasement in drywall.
Mass timber elements are defined in the Canadian building code as combustible construction. This could be a major stumbling block to the use of mass timber as a material in healthcare buildings. While recent changes in the Canadian building code now allow the use of mass timber in buildings up to 12 stories in height for residential and commercial occupancies, these new provisions do not extend to healthcare facilities, which still have restrictive code limits on combustible construction.
When designing healthcare buildings that are beyond the height and area limits of the code with combustible construction, performance-based design is used. This requires a fire engineer to holistically design the healthcare building such that the performance provided during a fire scenario meets or exceeds the performance that a code-compliant solution would have.
In addition to using encapsulation to provide a structural fire-resistance rating, the design team looks more broadly at the overall fire safety strategy of the building and how using a combustible structure may influence this. Any additional risks must be mitigated with compensating measures, such as an improved egress design, more reliable and robust suppression systems, and improved detection.
Encapsulation is often required for these high-consequence buildings to ensure that the mass timber structure itself does not keep burning if firefighters or sprinklers are unable to suppress the fire. While performance-based design can help maximize how much timber is exposed, the reality is that large parts of the structure will be concealed from view.
ROADBLOCK 3: INFECTION CONTROL
Another current impediment to the use of mass timber in healthcare facilities is the requirement for infection control. CSA Z8000 is the Canadian standard that governs the infection control requirements in healthcare facilities. This code states that materials and surfaces shall be appropriate to their location.
In high-risk areas such as operating rooms and intensive care units, surfaces are to be smooth and monolithic, and durable enough to withstand the additional cleaning and disinfection required. Exposed cellulose-based materials are not permitted due to their response to excessive moisture and sensitivity to wear. Surfaces must be easy to clean, resistant to microbial spread and growth, smooth and non-porous, and seamless.
These strict requirements set a high bar for healthcare facilities. Some authorities therefore reject the use of mass timber in healthcare. It is important not only to show that mass timber building systems can meet the challenges posed by structural requirements but also those surrounding infection control.
Timber is a natural material. Even engineered products such as CLT, which is fabricated from kiln-dried lamination stock, will always shrink and expand with moisture changes. This will cause checks in the surface of the wood elements. These, and other imperfections, will not meet the requirements of the clauses of CSA Z8000 as noted above.
However, concrete structures are subject to the same infection control requirements. Concrete is a porous material. All concrete floor slabs will crack due to shrinkage and flexure and are prone to spalling and creating dust. Untreated concrete surfaces are difficult to clean and disinfect. It is for this reason that even concrete is typically covered with epoxy flooring to meet the requirements of CSA Z8000.
This same approach can be used in mass timber construction. Keeping in mind that a concrete composite topping as outlined previously is typically part of any mass timber flooring system. The requirements to encapsulate mass timber for fire performance can be used to meet the requirements for infection control.
CONCLUSION
If encapsulation is the way forward for the use of mass timber in healthcare, then one may ask why bother? Why not continue using concrete systems that are well understood? If we cannot see the timber elements and experience their healing presence, are we wasting our time?
For Entuitive, our motivation rests in the sustainability aspect. If we can reduce the use of concrete by its partial replacement with timber, a renewable resource, we contribute to the protection of the environment. Sustainability and carbon sequestration are increasingly driving design. Local municipalities such as Vancouver are targeting a reduction of greenhouse gas emissions.

The need for further study is clear. The design community and government at several levels have a responsibility to explore the challenges and to question the status quo. The question is how we as a community take on this challenge.